
Journal of Emergency Medicine Thoracic Spine Compression Fracture After Taser Activation 2008
Download original document:
Document text
Document text
This text is machine-read, and may contain errors. Check the original document to verify accuracy.
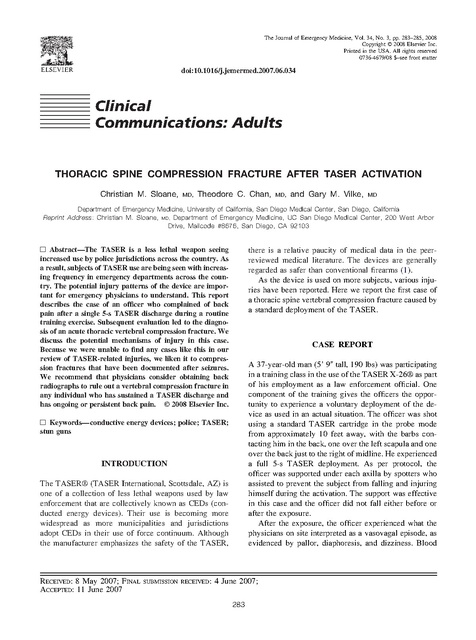
The Journal of Emergency Medicine, Vol. 34, No. 3, pp. 283–285, 2008 Copyright © 2008 Elsevier Inc. Printed in the USA. All rights reserved 0736-4679/08 $–see front matter doi:10.1016/j.jemermed.2007.06.034 Clinical Communications: Adults THORACIC SPINE COMPRESSION FRACTURE AFTER TASER ACTIVATION Christian M. Sloane, MD, Theodore C. Chan, MD, and Gary M. Vilke, MD Department of Emergency Medicine, University of California, San Diego Medical Center, San Diego, California Reprint Address: Christian M. Sloane, MD, Department of Emergency Medicine, UC San Diego Medical Center, 200 West Arbor Drive, Mailcode #8676, San Diego, CA 92103 e Abstract—The TASER is a less lethal weapon seeing increased use by police jurisdictions across the country. As a result, subjects of TASER use are being seen with increasing frequency in emergency departments across the country. The potential injury patterns of the device are important for emergency physicians to understand. This report describes the case of an officer who complained of back pain after a single 5-s TASER discharge during a routine training exercise. Subsequent evaluation led to the diagnosis of an acute thoracic vertebral compression fracture. We discuss the potential mechanisms of injury in this case. Because we were unable to find any cases like this in our review of TASER-related injuries, we liken it to compression fractures that have been documented after seizures. We recommend that physicians consider obtaining back radiographs to rule out a vertebral compression fracture in any individual who has sustained a TASER discharge and has ongoing or persistent back pain. © 2008 Elsevier Inc. there is a relative paucity of medical data in the peerreviewed medical literature. The devices are generally regarded as safer than conventional firearms (1). As the device is used on more subjects, various injuries have been reported. Here we report the first case of a thoracic spine vertebral compression fracture caused by a standard deployment of the TASER. CASE REPORT A 37-year-old man (5’ 9Љ tall, 190 lbs) was participating in a training class in the use of the TASER X-26® as part of his employment as a law enforcement official. One component of the training gives the officers the opportunity to experience a voluntary deployment of the device as used in an actual situation. The officer was shot using a standard TASER cartridge in the probe mode from approximately 10 feet away, with the barbs contacting him in the back, one over the left scapula and one over the back just to the right of midline. He experienced a full 5-s TASER deployment. As per protocol, the officer was supported under each axilla by spotters who assisted to prevent the subject from falling and injuring himself during the activation. The support was effective in this case and the officer did not fall either before or after the exposure. After the exposure, the officer experienced what the physicians on site interpreted as a vasovagal episode, as evidenced by pallor, diaphoresis, and dizziness. Blood e Keywords— conductive energy devices; police; TASER; stun guns INTRODUCTION The TASER® (TASER International, Scottsdale, AZ) is one of a collection of less lethal weapons used by law enforcement that are collectively known as CEDs (conducted energy devices). Their use is becoming more widespread as more municipalities and jurisdictions adopt CEDs in their use of force continuum. Although the manufacturer emphasizes the safety of the TASER, RECEIVED: 8 May 2007; FINAL ACCEPTED: 11 June 2007 SUBMISSION RECEIVED: 4 June 2007; 283 284 C. M. Sloane et al. Figure 1. Plain radiograph of thoracic spine demonstrating T7 compression fracture (arrow denotes fracture). pressure taken at the time was low (84/50 mm Hg) and pulse was 94 beats/min. The patient never lost consciousness. He was assisted to a position of comfort, which for him was supine on the floor with his legs flexed. He did not fall. His vagal symptoms resolved, but when he tried to get up he complained of severe midline thoracic back pain. When symptoms persisted after a period of observation, emergency medical services were accessed and the officer was transported to a local hospital for evaluation of continued back pain after voluntary TASER exposure. In the Emergency Department, the patient had normal vital signs but continued to complain of pain in the mid to low thoracic spine as well as the lumbar spine. Examination showed mild point tenderness over the spine at T7–T10 as well as L2–3. His neurologic examination was intact, including normal motor, sensory, and deep tendon reflexes. Plain films of the thoracic spine confirmed a compression fracture of T7 with anterior wedging (Figure 1). Lumbar films were negative. The radiologist also commented on diffuse osteopenia greater than expected for the patient’s age. A subsequent magnetic resonance imaging scan confirmed an acute compression fracture (Figure 2). The patient was treated with narcotic analgesia and non-operatively managed by an orthopedic spine specialist. His symptoms improved. The patient had reported no medical problems, no history of previous back pains or back issues, no medication use, and no history of frequent fractures or recurrent steroid use. It weighs approximately 18 ounces, and is powered by either NiCad batteries or high-output alkaline Duracell Ultra® batteries (The Gillette Company, Bethel, CT). The energy output of the device is 26 watts total, 1.76 joules per pulse, 36 milliamps, 50,000 volts. It uses an automatic timing mechanism to apply the electric charge for 5 s. When the trigger is depressed, a compressed nitrogen cartridge (1800 lb/in2) fires two probes at an initial velocity of 180 feet per second. The TASER delivers its electrical discharge energy through a sequence of dampened sine-wave current pulses each lasting about 11 ms. The electrical discharge is transmitted from the TASER gun through thin copper wires to the end probes. The probes, also known as barbs or darts, consist of a thick metal base and thin metal shaft with a barb on the end similar to a fish hook. They are designed to penetrate and stick in skin or clothing. The device will deliver its current and obtain the desired effect as long as the probes are within 2 inches of the victim’s skin. The manufacturer recommends 12–18 feet distance with the police model to obtain a minimum 4-inch spacing that optimizes obtaining the desired effect. The current TASER works by incapacitating one’s ability to maintain volitional control of the body by causing electro-physical, involuntary contraction of skel- DISCUSSION The device used in this event was the TASER X-26®. The X-26 is a handheld device resembling a handgun that is intended to be used on subjects up to 21 feet away. Figure 2. Magnetic resonance imaging scan of the thoracic spine demonstrating acute T7 compression fracture without spinal canal compromise (arrow denotes fracture). Spine Fracture after TASER Activation etal muscle tissue. It overrides the nervous system, resulting in loss of motor control by the subject. The TASER directly stimulates motor nerve and muscle tissue, causing incapacitation regardless of the subject’s mental focus, training, size, or drug intoxication state. Various injuries have been reported after the use of the TASER, the most controversial of which is death of a subject after a TASER activation. Causality has not been definitely linked solely to the TASER. Other injuries such as puncture wounds to the phalanges of the hands and the eye also have been reported (2– 4). There is one report of a pregnant woman who underwent a miscarriage days after receiving a TASER deployment (5). To our knowledge, no injuries have been reported relative to the musculoskeletal system not related solely to the barbs or penetration. In a search of the MEDLINE database, we were unable to find any other cases of a vertebral compression fracture as a result of a TASER deployment. The TASER creates intense involuntary contractions of skeletal muscle, causing the subject to lose the ability to directly control the actions of the voluntary muscles. This is an electrical effect and it terminates as soon as the electrical discharge is halted. We feel confident that this injury was a result of the TASER deployment. The patient had no complaints of back pain before the deployment and denied prior back injuries. The pain began immediately after the exposure. The pain was severe enough to cause a vagal reaction. The magnetic resonance imaging scan confirmed the acute nature of the injury. How did this occur in the absence of a fall? We suspect that the location of the barb contact points being in the back across the relatively large paraspinous muscle groups may have led to the abrupt forceful contractions of those muscles or other muscles of the torso, resulting in an acute compression fracture of the vertebral body. This is similar to the proposed mechanisms for compression fractures that have been reported after seizures (6 – 8). It is interesting that the radiologist commented on 285 osteopenia in this young man’s radiographs, which, if confirmed, may have placed him at increased risk. It is documented that in epileptics who sustain compression fractures after a seizure, decreased bone mineral density is often to blame. In these cases, it is often secondary to the negative effects of long-term anticonvulsant therapy on bone mineral density (7). We suspect that this type of injury has occurred before but has never been reported, either because the individuals never sought medical attention or radiographs were not performed and the symptoms attributed to a strain. The natural course of many slight compression fractures is such that they improve without the need for any intervention. TASERs are a less lethal technology that have reduced gun use by police officers, but can be associated with physical injuries similar to any other less lethal weapons. Given this current case report, we recommend that physicians consider obtaining back radiographs to rule out a vertebral compression fracture in any individual who has sustained a TASER discharge and has ongoing or persistent back pain. REFERENCES 1. Ordog G, Wasserberger J, Schlater T, et al. Electronic gun (Taser) injuries. Ann Emerg Med 1987;16:73– 8. 2. Chen SL, Richard CK, Murthy RC, Lauer AK. Perforating ocular injury by Taser. Clin Experiment Ophthalmol 2006;34:378 – 80. 3. Dearing M, Lewis TJ. Foreign body lodged in distal phalanx of left index finger-taser dart. Emerg Radiol 2005;11:364 –5. 4. Ng W, Chehade M. Taser penetrating ocular injury. Am J Ophthalmol 2005;139:713–5. 5. Mehl LE. Electrical injury from Tasering and miscarriage. Acta Obstet Gynecol Scand 1992;71:118 –23. 6. Roohi F, Fox A. Burst fracture of the first lumbar vertebra and conus-cauda syndrome complicating a single convulsive seizure: a challenge of diagnosis in the Emergency Department. J Emerg Med 2006;31:381–5. 7. Takahashi T, Tominaga T, Shamoto H, Shimizu H, Yoshimoto T. Seizure-induced thoracic spine compression fracture: case report. Surg Neurol 2002;58:214 – 6; discussion 216 –7. 8. McCullen GM, Brown CC. Seizure-induced thoracic burst fractures. A case report. Spine 1994;19:77–9.