
The Prevalence and Severity of Mental Illness Among California Prisoner's on the Rise, Stanford Justice Advocacy Project, 2017
Download original document:
Document text
Document text
This text is machine-read, and may contain errors. Check the original document to verify accuracy.
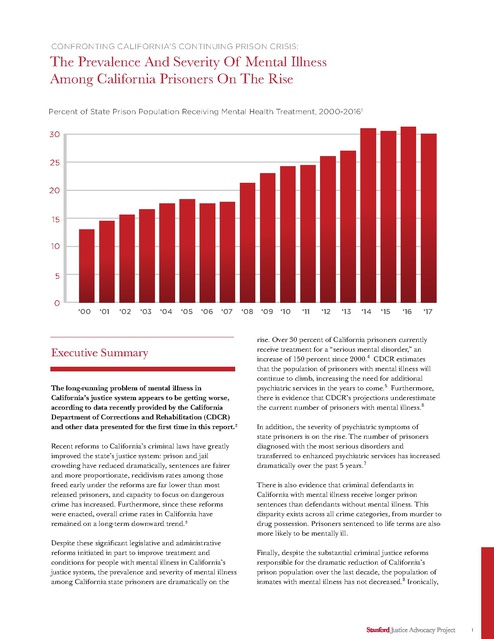
CONFRONTING CALIFORNIA’S CONTINUING PRISON CRISIS: The Prevalence And Severity Of Mental Illness Among California Prisoners On The Rise Percent of State Prison Population Receiving Mental Health Treatment, 2000-20161 30 25 20 15 10 5 0 ‘00 ‘01 ‘02 ‘03 ‘04 ‘05 ‘06 ‘07 Executive Summary The long-running problem of mental illness in California’s justice system appears to be getting worse, according to data recently provided by the California Department of Corrections and Rehabilitation (CDCR) and other data presented for the first time in this report.2 Recent reforms to California’s criminal laws have greatly improved the state’s justice system: prison and jail crowding have reduced dramatically, sentences are fairer and more proportionate, recidivism rates among those freed early under the reforms are far lower than most released prisoners, and capacity to focus on dangerous crime has increased. Furthermore, since these reforms were enacted, overall crime rates in California have remained on a long-term downward trend.3 Despite these significant legislative and administrative reforms initiated in part to improve treatment and conditions for people with mental illness in California’s justice system, the prevalence and severity of mental illness among California state prisoners are dramatically on the ‘08 ‘09 ‘10 ‘11 ‘12 ‘13 ‘14 ‘15 ‘16 ‘17 rise. Over 30 percent of California prisoners currently receive treatment for a “serious mental disorder,” an increase of 150 percent since 2000.4 CDCR estimates that the population of prisoners with mental illness will continue to climb, increasing the need for additional psychiatric services in the years to come.5 Furthermore, there is evidence that CDCR’s projections underestimate the current number of prisoners with mental illness.6 In addition, the severity of psychiatric symptoms of state prisoners is on the rise. The number of prisoners diagnosed with the most serious disorders and transferred to enhanced psychiatric services has increased dramatically over the past 5 years.7 There is also evidence that criminal defendants in California with mental illness receive longer prison sentences than defendants without mental illness. This disparity exists across all crime categories, from murder to drug possession. Prisoners sentenced to life terms are also more likely to be mentally ill. Finally, despite the substantial criminal justice reforms responsible for the dramatic reduction of California’s prison population over the last decade, the population of inmates with mental illness has not decreased.8 Ironically, 1 these reforms were largely initiated on behalf of inmates with mental illness suffering under unconstitutional treatment conditions.9 Among California’s ten largest counties, Alameda County sends the largest percentage of inmates with mental illness to state prison (42 percent) and Orange County sends the smallest (24 percent).12 This report contains new and updated data about the growing problem of mental illness in California’s justice system and describes how prisoners with mental illness do not benefit from some of the most important criminal justice reforms enacted in the state in recent years. • Recent reforms may inadvertently contribute to problems facing inmates with mental illness: Recent sentencing reforms that condition release on in-prison behavior contribute to the increasing population of prisoners with mental illness. Disciplinary rules and access to rehabilitative programs fail to adequately account for psychiatric conditions. KEY FINDINGS • The number of prisoners with mental illness in California is on the rise: While the overall state prison population has decreased dramatically, the number of prisoners with mental illness continues to climb and is expected to grow in the years ahead. Over the past decade, the percentage of state prisoners with mental illness has increased by 77 percent.10 • Defendants with mental illness in state hospitals are deprived of the benefits of recent sentencing reforms: Hundreds of nonviolent defendants with mental illness confined in state hospitals are denied eligibility for early release under sentencing reforms available to prisoners with the same criminal history but no mental illness.13 • There are insufficient community mental health treatment services: The total number of hospital beds in communities throughout California for individuals who need short-term acute psychiatric care has decreased 30 percent since 1995.14 • The severity of psychiatric symptoms among California prisoners is also on the rise: Since 2012, the number of prisoners requiring enhanced mental health services has increased by over 60 percent.11 • Defendants with mental illness receive longer prison sentences: On average, prisoners with mental illness in California receive sentences that are 12 percent longer than prisoners convicted of the same crimes but without mental health diagnoses. • Community mental health treatment is more effective and less expensive than incarceration: The annual cost of incarcerating an average state prisoner in California is over $70,000, not including mental healthcare costs, while the cost of treating a person with mental illness in the community is approximately $22,000.15 • Some counties send a disproportionate number of defendants with mental illness to state prison: Increase of Prisoners in Enhanced Outpatient (EOP) Care, 2012-201616 7000 6500 6000 5500 5000 4500 MAY 2012 SEPT JAN 2013 MAY SEPT JAN 2014 MAY SEPT JAN 2015 MAY SEPT JAN MAY SEPT 2016 2 Prevalance And Acuity Of Mental Illness Among State Prisoners On The Rise Prevalence of Mental Illness among Latino Prisoners (2017) Percentage of Overall Prison Population % Percentage of Mental Health Treatment Population 50 40 Over the past decade, California’s overall prison population has decreased by approximately 40,000 inmates, or 25 percent. Over the same period of time, the raw number of prisoners with mental illness increased by 25 percent. CDCR anticipates need for additional psychiatric treatment capacity in the years to come.17 CDCR also reports that current prison health care services are understaffed.18 In 2000, CDCR identified 12 percent of the state prison population as mentally ill, diagnosed with serious mental disorders, including schizophrenia, psychotic, and bi-polar disorders. Today, that number has grown to over 32 percent of the state’s prison population. These figures may even underestimate the overall prevalence of mental illness in California’s prisons. For example, Latino inmates constitute the largest group of prisoners by race in California prisons 30 20 10 0 NO. OF PRISONERS AND % OF TREATMENT POPULATION LEVEL OF CARE Correctional Clinical Case Management System (CCCMS) • Treatment for “serious mental disorder,” according to certain DSM Axis I diagnoses (e.g. schizophrenia, psychotic disorder, bipolar disorder). • Treatment includes medication, individual and group therapy. Enhanced Outpatient Program (EOP) • Segregated housing. • Treatment for acute onset or significant decompensation, including delusional thinking, hallucinations, vegetative affect. • Global Assessment Score less than 50. • Treatment includes medication, individual and group therapy, at least 10 hours per week of structured therapeutic activities. Inpatient at Dept. Mental Health Intermediate and Acute Care • Acute exacerbation of a chronic major mental illness, marked impairment, and dysfunction in most areas. • Highly structured in-patient psychiatric care with 24-hour nursing supervision. • Danger to self or others. • May require neurological/neuropsychological consultation. • Anticipated discharge within 30-45 days. Mental Health Crisis Bed • In-patient psychiatric care, with 10-day maximum stay. • Continuous therapeutic assistance to inmate-patients whose condition requires 24 hours or more to achieve stabilization. • Danger to self or others. • Global Assessment Score less than 30. • Treatment to control and alleviate symptoms with emergency medication if necessary. 29,062 77% 7,408 20% 1,093 344 3% 1% 3 yet appear to be significantly underrepresented among the population of prisoners with mental illness. Latino prisoners make up over 43 percent of the overall prison population but only 27 percent of inmates with mental illness. The severity of inmates’ mental illness is also on the rise. Since 2012, the number of prisoners referred for intensive psychiatric treatment as part of CDCR’s Enhanced Outpatient Services (EOP) has increased by 60 percent. At the same time, there appears to be a deficit of psychiatric staffing in CDCR. As of 2015, 32 percent of psychiatrist positions in CDCR remain unfilled.19 As recently as April 19, 2017 a federal court found ongoing delays in transferring prisoners who require acute and enhanced mental health treatment to appropriate psychiatric care services. The court ordered the CDCR to remedy the situation by May 15, 2017 or face financial penalties.20 Even the United States Supreme Court has acknowledged that inmates with mental illness in California prisons often get worse instead of better.21 Administrative penalties (including placement in secure and segregated confinement) exacerbate mental illness and lead to a downward spiral of increased symptoms, noncompliant behavior, and psychiatric decompensation.22 The Supreme Court noted that the suicide rate among California prisoners was nearly 80 percent higher than the national average for prisoner populations and that over 72 percent of suicides in California’s state prisons at the time were “most probably foreseeable and/or preventable.”23 Inmates With Mental Illness Serve Longer Prison Sentences For The Same Crimes California defendants with mental illness are sentenced to longer prison terms than defendants without mental illness convicted of the same crimes. On average, the sentences for prisoners with mental illness are 12 percent longer than other prisoners. This disparity exists across all crime categories, from murder to simple drug possession. Prisoners sentenced to life terms are also more likely to be mentally ill. Prisoners with Mental Illness Receive Longer Sentences (Feb. 2017) MENTALLY ILL NON-MENTALLY ILL Child Molestation Kidnapping Robbery Burglary Assault/Battery Marijuana Sales Weapon possesion Petty Theft 0 50 100 150 200 250 The problem is compounded because prisoners with mental illness are more likely to be denied parole and lose other opportunities for early release based on good behavior.24 Recent California state court decisions have also contributed to the problem. For example, a California appellate court recently ruled that nonviolent defendants confined in mental hospitals are not entitled to the benefits of voter-enacted reforms. In People v. Dobson, the Court ruled that defendants with mental illness who committed nonviolent crimes falling under the Three Strikes law and were found not guilty by reason of insanity are not eligible to seek reduction in confinement under the Three Strikes Reform Act (Proposition 36).25 By contrast, prisoners without mental illness convicted of the exact same crimes and with the exact same criminal histories may be released early under the reform.26 Other state courts have ruled that prisoners with mental illness are ineligible for shorter sentences due to in-prison disciplinary infractions directly related to mental illness (including prison rule violations for attempted suicide) despite federal court rulings questioning CDCR’s prison disciplinary system in its application to prisoners with mental illness.27 Although the problem of prisoners with mental illness is largely a statewide issue, disparities appear among California’s 58 counties in response to crimes committed by defendants with mental illness. For example, among the ten largest counties in California, 42 percent of defendants convicted and sentenced to prison in Alameda County have a mental illness, compared to 24 percent of defendants from Orange County. It is not clear why some counties send a larger proportion of defendants with mental illness than others. Even counties with robust behavioral health courts and diversion programs, like San Francisco, send a higher percentage of mentally ill defendants to prison compared to the state average. 4 Percentage of Prisoners with Mental Illness, Fifteen Largest Counties (Feb. 2017). 42% 40% 38% 36% 34% 32% 30% 28% SAN FRANCISCO ALAMEDA SACRAMENTO CONTRA COSTA SAN DIEGO FRESNO KERN SAN MATEO LOS ANGELES SANTA CLARA RIVERSIDE VENTURA 20% ORANGE 22% SAN MATEO 24% SAN BERNARDINO 26% Recent Criminal Justice Reforms Leave Behind Prisoners With Mental Illness It is ironic that recent reforms to California’s criminal justice system have neglected prisoners with mental illness who, as a group, were largely responsible for initiating the wave of reform in the first place. In 1995, prisoners with mental illness won a class action lawsuit against the California prison system for failing to provide the most rudimentary level of psychiatric care.28 After decades of failed settlement negotiations and attempted remediation by the state, the case ended up in the United States Supreme Court, which in 2011 affirmed a dramatic reduction to the state’s prison population. The explicit purpose of the prison reduction order was to improve treatment of psychiatrically and medically vulnerable inmates.29 Since the Supreme Court’s decision, California’s overall prison population has decreased by over 25 percent while prisoners with mental illness seem to be left behind. Coleman and Plata litigation (1991) In 1991, a plaintiff class including “all inmates with serious mental disorders who are now or who will in the future be confined within the California Department of Corrections” sued then-Governor Pete Wilson and other state officials in the federal district court for the Eastern District of California over alleged constitutional violations within the state prison system. After a 39-day trial, the court found in Coleman v. Wilson “overwhelming evidence of the systematic failure to deliver necessary care to mentally ill inmates.”30 three-judge panel ruled that prison crowding was the direct cause of unconstitutional conditions for mentally and physically ill inmates and ordered that the state reduce its prison population to 137.5 percent of overall design capacity. In 2011, the United States Supreme Court upheld the prison downsizing order in a landmark decision, now titled Brown v. Plata. The Court justified its ruling by noting that prisoners with mental illness in California were being denied fundamental rights to human dignity and directed the state to meet the prison population cap ordered by the three-judge panel “without further delay.”31 AB 109: Public Safety Realignment (2011) In response to the Coleman and Plata litigation, the California legislature enacted Assembly Bill 109, known as “Public Safety Realignment.” The legislation began California’s prison downsizing process in earnest by implementing several reforms designed to reduce the prison population and improve conditions for inmates with mental and physical illnesses. The new law provided that defendants convicted of most nonviolent crimes, and parolees who violated the terms of their release, would serve their sentences in county jails rather than state prison. In addition, the legislature directed that most inmates released from state prison be supervised by county probation departments rather than state parole officers. The legislation also allocated billions of dollars in new funding to county governments to help absorb the cost of new criminal justice obligations. Within six months, the state prison population dropped by more than 21,000 inmates.32 In 2009, after years of attempted mediation, a special 5 Proposition 36: Three Strikes Reform (2012) In 2012, California voters enacted Proposition 36, the Three Strikes Reform Act, amending the state’s recidivist sentencing law. At the time, most prisoners sentenced under the Three Strikes law were serving life sentences for nonviolent crimes. Proposition 36 provided that life sentences could only be imposed for serious or violent third strike offenses. The ballot measure also provided a mechanism for current nonviolent Three Strikes prisoners to petition for early release if they could demonstrate to a court that they no longer posed “an unreasonable risk of danger to public safety.” In making this determination, courts are instructed to consider the petitioner’s prison disciplinary record and record of rehabilitation.33 Since Proposition 36 was enacted, more than 2,200 nonviolent prisoners sentenced to life under the Three Strikes law have been released.34 The recidivism rate of those released under the initiative is more than four times lower than the average inmate released from prison in California.35 Proposition 47: Safe Neighborhoods and Schools Act (2014) In 2014, voters approved Proposition 47, the Safe Neighborhoods and Schools Act, further amending California sentencing laws. Among other things, Proposition 47 reduced the punishment for six common nonviolent crimes from potential felonies to mandatory misdemeanors. Proposition 47 also provided a mechanism for early release of those serving felony sentences for the targeted crimes unless a petitioner posed a public safety risk.36 More than 10,000 inmates convicted of petty offenses have been released from prison and county jails under the reform. Again, the recidivism rate of those released early under this ballot measure is well below the state’s average recidivism rate.37 Senate Bill 260 and 261: Youth Offender Parole (2013-15) In 2013, the California legislature enacted Senate Bill 260 to provide an opportunity for early parole for certain prisoners who were under the age of 18 when they committed their crimes. In 2015, the legislature enacted Senate Bill 261 expanding the new parole opportunity to prisoners who were under the age of 23 when they committed their crimes. As of March 2017, over 650 prisoners have been granted parole and released under these measures.38 Proposition 57: Public Safety and Rehabilitation Act (2016) In 2016, voters enacted yet another criminal justice reform, Proposition 57, the Public Safety and Rehabilitation Act, which was sponsored by Governor Jerry Brown. Proposition 57 provides early parole for certain nonviolent prisoners and instructs CDCR to expand opportunities for prisoners to earn time off their sentences by participating in rehabilitative prison programing. Proposition 57 also amends rules for charging juveniles in adult court. Proposition 57 is estimated to reduce the state prison population by 9,500 inmates in the next five years.39 People v. Dobson: Denying Reform To Inmates With Mental Illness Last year, in People v. Dobson, the California Court of Appeal ruled that defendants found not guilty by reason of insanity are not eligible for sentence reductions under Proposition 36.40 The case involves Steven Dobson, who in 1998 confessed to the crime of joyriding and pleaded not guilty by reason of insanity. The Court committed Mr. Dobson to Patton State Hospital for the length of his prison sentence—which, in this case, was 25 years-to-life because Mr. Dobson was charged under the Three Strikes law. Today the maximum sentence for this crime, taking into account Mr. Dobson’s criminal history, is six years, and prisoners convicted under the Three Strikes law may petition for early release 41 under Propositions 36 and 47. Nonetheless, the Court of Appeal ruled that Mr. Dobson was not eligible for resentencing consideration, even if he posed no risk to public safety. The Court determined that Proposition 36 applied only to “prisoners” and not to “patients” in state hospitals—even if the patient committed the exact same crime as the prisoner. 6 How Prisoners With Mental Illness Are Left Behind By California’s Reforms There are several reasons why prisoners with mental illness are not reaping the benefits of many of the reforms that have been enacted over the past decade, which were largely inspired by their poor treatment and groundbreaking 1991 legal action. First, almost all of the recent reforms enacted in California emphasize inmates’ in-prison behavior when evaluating suitability for early release. Reforms that provide early release and early parole consideration establish that a prisoner’s suitability for release depends in part on the presence or absence of prison rule violations committed by the inmate under review.42 However, as previously discussed, prison conditions are likely to exacerbate a prisoner’s existing mental illness and deteriorating behavior. For example, CDCR regulations provide disciplinary sanctions for prisoners who attempt suicide.43 This sanction results in loss of privileges within prison, loss of custody credits that can reduce the inmate’s sentence, loss of rehabilitative programing opportunities, and an increase in the prisoner’s custody security level. Even prisoners with mental illness who do not commit rule violations and who diligently comply with psychiatric treatment may have been disadvantaged. These inmates were frequently unable to participate in rehabilitative programming, such as vocational training or educational classes, because of conflicts with their treatment scheduleand mental health programs. The recently-approved emergency regulations implementing Proposition 57 provide that inmates with mental illness will earn credit for participating in their structured therapeutic activity, among other rehabilitative programs. 46 Cost of Mental Health Treatment CDCR Mental Health Crisis Bed $345K State Mental Hospital Bed $218K Cost of Average CDCR Inmate $75.2K Opportunities For Community Based Mental Health Services Research shows that community based psychiatric treatment is frequently more effective and significantly less expensive than in-prison treatment at preventing crime and reducing incarceration rates for people with mental illness.44 There are a number of public programs supporting various community treatment options in California. Community-Based Mental Health Bed $21.9K Marginal Cost of Parolee Supervision w/Mental Health Treatment $7.9K The Affordable Care Act (ACA): The ACA extended health coverage, including mental health services, to more than 4.7 million low-income 7 Californians.45 Reducing federal funds, amending the ACA, or cutting eligibility to Medi-Cal threatens the mental health care of indigent Californians, and would likely create new pressures on the criminal justice system. and out-patient services, while serving as a hub for police and community based mental health treatment programs in San Francisco.48 Institute for Mental Disease (IMD) Exclusion: Federal law has severely restricted the availability of residential mental health treatment programs. Under the Institute for Mental Disease (IMD) exclusion in the original 1965 federal Medicaid law, residential mental health facilities with more than 16 beds are prohibited from receiving federal funding. The exclusion was intended to avoid large “Cuckoo’s Nest” mental health hospitals and place primary responsibility for psychiatric services on state and county governments. The exclusion has effectively prohibited Medi-Cal-funded residential mental health treatment. Proposition 63: Mental Health Services Act: In 2004, California voters approved Proposition 63, which levied a one percent tax on personal incomes over $1 million to pay for mental health services. In 2013, state lawmakers passed Senate Bill 82, distributing income generated by Proposition 63 to counties to improve mental health treatment services. In 2016, lawmakers enacted Assembly Bill 1618, the No Place Like Home Act, providing another $2 billion from Proposition 63 to build housing for those with mental illness.47 Proposed San Francisco Behavioral Health Justice Center (BHJC): San Francisco police receive approximately 20,000 emergency calls for people in mental health crises every year. Over 35 percent of San Francisco jail inmates receive mental health services, and the number of mental health crisis beds in the county general hospital was cut by two-thirds in recent years. In January 2016, San Francisco District Attorney George Gascón proposed a new kind of facility to help address this problem using city money already set aside for a new jail building. The program would serve as a 24-hour facility for police to redirect suspects with mental illness away from traditional jail and provide different levels of services, depending on the criminal charges involved and the severity of an individual’s psychiatric diagnosis. As envisioned, the BHJC would include a secure level of care for the most serious cases, as well as residential treatment, Cost of Incarceration Compared to Residential Community Treatment49 30K 25K Contract rate for out-of-state prison bed 20K 15K Residential Community Treatment 10K 5K 0 CONCLUSION Despite success in reducing prison overcrowding in California, recent reforms have failed to adequately address the role of mental illness in the criminal justice system. The number of prisoners with mental illness in California is on the rise and the seriousness of their psychiatric conditions is worsening. Furthermore, the state prison system remains under federal court order for insufficient staffing, improper security procedures for inmates with mental illness, and failing to provide adequate psychiatric treatment. Many reforms are needed to address the intersection between mental illness and criminal justice. This report is intended to highlight the growing problem in California, help provide new evidence and context surrounding the state’s mental health prison crisis, and encourage policymakers and stakeholders to develop and embrace new and lasting solutions to one of the most vexing issues facing California’s justice system. 8 1 “New Challenges Raised by Decarceration: Discrimination in Population Reduction Tactics,” presented by Michael Bien at Western Society of Criminology (Feb. 2017) (citing HC-POP Summary of Outpatient Population (enclosure 6A, Coleman monthly report), CDCR monthly population report archive). 18 2 20 Unless otherwise noted, all data in this report were provided by CDCR in February 2017. For purposes of this report, a “prisoner receiving mental health treatment” or “prisoner with mental illness” means the prisoner was reported as receiving care in the CDCR Mental Health Delivery System as of February 6, 2017. 3 See Cal. Dept. of Justice, California Justice Information Division, “Crime in California, 2015.” 4 Cal. Dept. of Corrections and Rehabilitation and Cal. Correctional Health Care Services, “Mental Health Bed Need Study,” (Jan. 8, 2016). Coleman, Doc. No. 5564, “Special Master’s Report on the Status of Mental Health Staffing and the Implementation of Defendant’s Staffing Plan,” (filed Feb. 6, 2017). 19 Id. Coleman, Doc. No. 5610, “Order,” (filed Apr. 19, 2017). 21 See Plata, 563 U.S. 493. 22 See Jeffrey Metzner and Jamie Fellner, “Solitary Confinement and Mental Illness in U.S. Prisons: A Challenge for Medical Ethics,” in Health and Human Rights in a Changing World (2013). 23 Plata, 563 U.S. at 504. 24 5 See, e.g., People v. Nolkemper, Los Angeles Sup. Ct. Case No. LA03006001 (Nov. 3, 2016) (finding petitioner unsuitable for release based on prison rule violations directly related to petitioner’s mental illness). 6 25 Id. See, e.g., Doris James and Lauren Glaze, “Mental Health Problems of Prison and Jail Inmates,” U.S. Department of Justice, Bureau of Justice Statistics (Dec. 2006) (reporting that 56 percent of state prisoners and 64 percent of jail inmates nationwide had a recent history or current symptoms of a mental health problem). See, e.g., People v. Dobson, 245 Cal. App. 4th 310 (2016) (holding that offenders confined in state mental hospitals are ineligible for certain sentencing reforms). 26 Id; Cal. Penal Code § 1170.126. 7 27 8 28 9 29 “New Challenges Raised by Decarceration,” M. Bien at Western Society of Criminology (Feb. 2017). Id. See generally Brown v. Plata, 563 U.S. 493 (2011); Coleman v. Wilson, 912 F. Supp. 1282 (E.D.CA 1995); see also Jonathan Simon, “Mass Incarceration on Trial: A Remarkable Court Decision and the Future of Prisons in America,” (The New Press 2014). 10 See “New Challenges Raised by Decarceration,” M. Bien at Western Society of Criminology (Feb. 2017). 11 CDCR and CCHCS, “Mental Health Bed Need Study,” (Jan. 8, 2016). 12 This does not account for the fact that the prevalence of mental illness differs between counties. Among the largest counties in California, Contra Costa county has the highest percentage of Medi-Cal enrollees receiving mental health services (7.2%) and Orange county has the lowest (3.4%). See Behavioral Health Concepts, “Medi-Cal Specialty Mental Health: External Quality Review, MHP Final Report, 2015-16,” (Jan. 2016). 13 Dobson, 245 Cal. App. 4th 310. 14 Cal. Hospital Association, “Psychiatric Inpatient Bed Data,” (Oct. 1, 2013). 15 Legislative Analyst’s Office, “How Much Does It Cost to Incarcerate an Inmate?” (Dec. 2016); Judicial Council of California, “Task Force for Criminal Justice Collaboration on Mental Health Issues: Final Report,” (Apr. 2011). 16 “New Challenges Raised by Decarceration,” M. Bien at Western Society of Criminology (Feb. 2017). 17 CDCR and CCHCS, “Mental Health Bed Need Study,” (Jan. 8, 2016). Brown v. Coleman, 28 F. Supp. 3d 1068 (E.D.CA. 2014); Nolkemper, Los Angeles Sup. Ct. Case No. LA030060-01. Coleman v. Wilson, 912 F. Supp. 1282 (E.D.CA. 1995). Plata, 563 U.S. 493. 30 Coleman, 912 F. Supp. at 1316. 31 Plata, 563 U.S. at 545. 32 Cal. Dept. of Finance, “California Budget Summary 2017-18, Public Safety,” (Jan. 2017). 33 Cal. Penal Code § 1170.126. 34 Plata, Case No. 2:90-cv-00520, Doc. No. 2931, “Defendants’ March 2017 Status Report in Response to February 10, 2014 order,” (filed Mar. 15, 2017). 35 Erik Eckholm, “Out of Prison and Staying Out After 3rd Strike in California,” The New York Times (Feb. 26, 2015). 36 Cal. Penal Code § 1170.18. 37 Stanford Law School, “Proposition 47 Progress Report: Year One Implementation,” (Oct. 2015). 38 Plata, Case No. 2:90-cv-00520, Doc. No. 2931, “Defendants’ March 2017 Status Report in Response to February 10, 2014 order,” (filed Mar. 15, 2017). 39 Cal. Dept. of Finance, “California Budget Summary 2017-18, Public Safety,” (Jan. 2017). 40 Dobson, 245 Cal. App. 4th 310. 9 41 See Cal. Penal Code §§ 1170.126, 1170.18. 42 Id. 43 See Tit. 15 CCR § 3315(a)(2)(W). CDCR’s disciplinary rules were revised in 2015 to require mental health assessments and mitigate penalties if the violation was caused by the inmate’s mental illness. (May 4, 2015 Stipulated Response and Order, Coleman Docket No. 5305.) 44 Judicial Council of California, “Task Force for Criminal Justice Collaboration on Mental Health Issues: Final Report,” (Apr. 2011). 45 Cal. Dept. of Health Care Services, “Affordable Care Act,” (2017). 46 According to the LAO, the marginal cost of incarcerating a CDCR inmate may be calculated in several different ways. The average annual cost of incarcerating a CDCR inmate is $75,210 (not including mental health costs); the marginal rate of housing an additional person in a state-owned prion is approximately $10,000 per year (not including mental health costs); the average marginal cost of staffing for inmates with mental illness is approximately an additional $6,800 per inmate annually (not including medication). In addition, note that according to CDCR regulations inmates should not be housed in Mental Health Crisis Beds (MHCBs) for more than 10 days, although in some cases inmates may be housed in these beds for longer periods of time. Data provided by the Legislative Analyst’s Office (Apr. 2017). 47 Cal. Assembly Bill 1618, Chapter 43, Statutes of 2016. 48 Craig Haney, et. al., “Justice That Heals: Promoting Behavioral Health, Safeguarding the Public and Ending Our Overreliance on Jails,” (Jun. 2016). 49 See CDCR, “An Update to the Future of California Corrections,” (Jan. 2016); Judicial Council of California, “Task Force for Criminal Justice Collaboration on Mental Health Issues: Final Report,” (Apr. 2011). 10