
Taser Cardiac Monitoring of Subjects Exposed to Taser Ucsd Emergency Medicine
Download original document:
Document text
Document text
This text is machine-read, and may contain errors. Check the original document to verify accuracy.
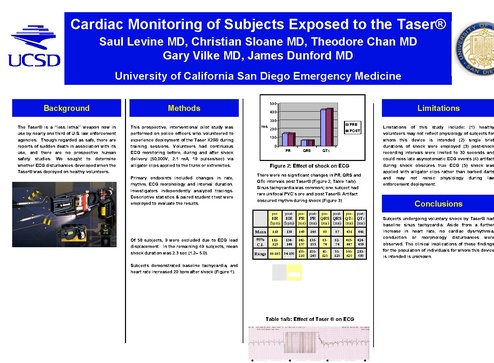
Cardiac Monitoring of Subjects Exposed to the Taser® Saul Levine MD, Christian Sloane MD, Theodore Chan MD Gary Vilke MD, James Dunford MD University of California San Diego Emergency Medicine Background 500 Methods Limitations 400 300 The Taser® is a “less lethal” weapon now in use by nearly one third of U.S. law enforcement agencies. Though regarded as safe, there are reports of sudden death in association with its use, and there are no prospective human safety studies. We sought to determine whether ECG disturbances developed when the Taser® was deployed on healthy volunteers. This prospective, interventional pilot study was performed on police officers who volunteered to experience deployment of the Taser X26® during training sessions. Volunteers had continuous ECG monitoring before, during and after shock delivery (50,000V, 2.1 mA, 19 pulses/sec) via alligator clips applied to the trunk or extremities. Primary endpoints included changes in rate, rhythm, ECG morphology and interval duration. Investigators independently analyzed tracings. Descriptive statistics & paired student t test were employed to evaluate the results. ms 0 PR QRS Figure 2: Effect of shock on ECG post- pre- post- pre- 118 138 149 146 69 67 431 441 112125 134144 142157 136155 6374 6274 415447 424458 100Range 66-160 94-190 210 100240 40120 50120 350620 283580 ∆ HR (bpm) ∆ PR (ms) ∆ QRS (ms) ∆ QTc (ms) <0.0001 0.22 0.35 0.19 -24.6 to -14.5 -2.25 to 9.47 -1.7 to 4.7 -26.4 to 5.5 -60 to 40 -30 to 20 -110 to 145 135 130 Range -1 to 72 138 125 118 Table 1a/b: Effect of Taser ® on ECG 110 105 POST-SHOCK Limitations of this study include: (1) healthy volunteers may not reflect physiology of subjects for whom this device is intended (2) single brief durations of shock were employed (3) post-shock recording intervals were limited to 30 seconds and could miss late asymptomatic ECG events (4) artifact during shock obscures true ECG (5) shock was applied with alligator clips rather than barbed darts and may not mimic physiology during law enforcement deployment. Conclusions post- 95% C.I. Pvalue 95% C.I. PRE-SHOCK pre- Mean Subjects demonstrated baseline tachycardia, and heart rate increased 20 bpm after shock (Figure 1). HR 120 (bpm) 115 post- HR HR PR PR QRS QRS QTc QTc (bpm) (bpm) (ms) (ms) (ms) (ms) (ms) (ms) Of 58 subjects, 9 were excluded due to ECG lead displacement. In the remaining 49 subjects, mean shock duration was 2.3 sec (1.2– 5.0). 140 QTc There were no significant changes in PR, QRS and QTc intervals post Taser® (Figure 2, Table 1a/b). Sinus tachycardia was common; one subject had rare unifocal PVC’s pre and post Taser®. Artifact obscured rhythm during shock (Figure 3) Results Researcher physician enjoying Taser ® with police training staff POST 100 pre- Taser X-26® PRE 200 Subjects undergoing voluntary shock by Taser® had baseline sinus tachycardia. Aside from a further increase in heart rate, no cardiac dysrhythmia, conduction or morphology disturbances were observed. The clinical implications of these findings for the population of individuals for whom this device is intended is unknown. Disclosures This study was accomplished without outside funding Acknowledgements Special thanks goes to the San Diego Police Department for allowing this study to be performed during scheduled officer training and to the San Diego Fire Rescue Department for providing ECG